Supported by:
Daily cone beam CTs (CBCTs) provide superior representation of patient anatomy at the time of treatment compared to the conventional planning CT. To assess the need for replanning, it should be possible to compute the dose based on the daily CBCT images. However, the quality of CBCT images is often sub-optimal in comparison to CT images.
|
CBCT images often suffer from artifacts and an unstable relationship between CBCT intensities and electron densities and therefore are not well-suited for dose computation. To overcome this challenge, RayStation* utilizes two advanced algorithms to create synthetic CTs, using the daily CBCT and the planning CT as input. This results in increased dose computation accuracy, which is crucial for establishing more reliable adaptive workflows in radiation therapy. |
BENEFITS:
|
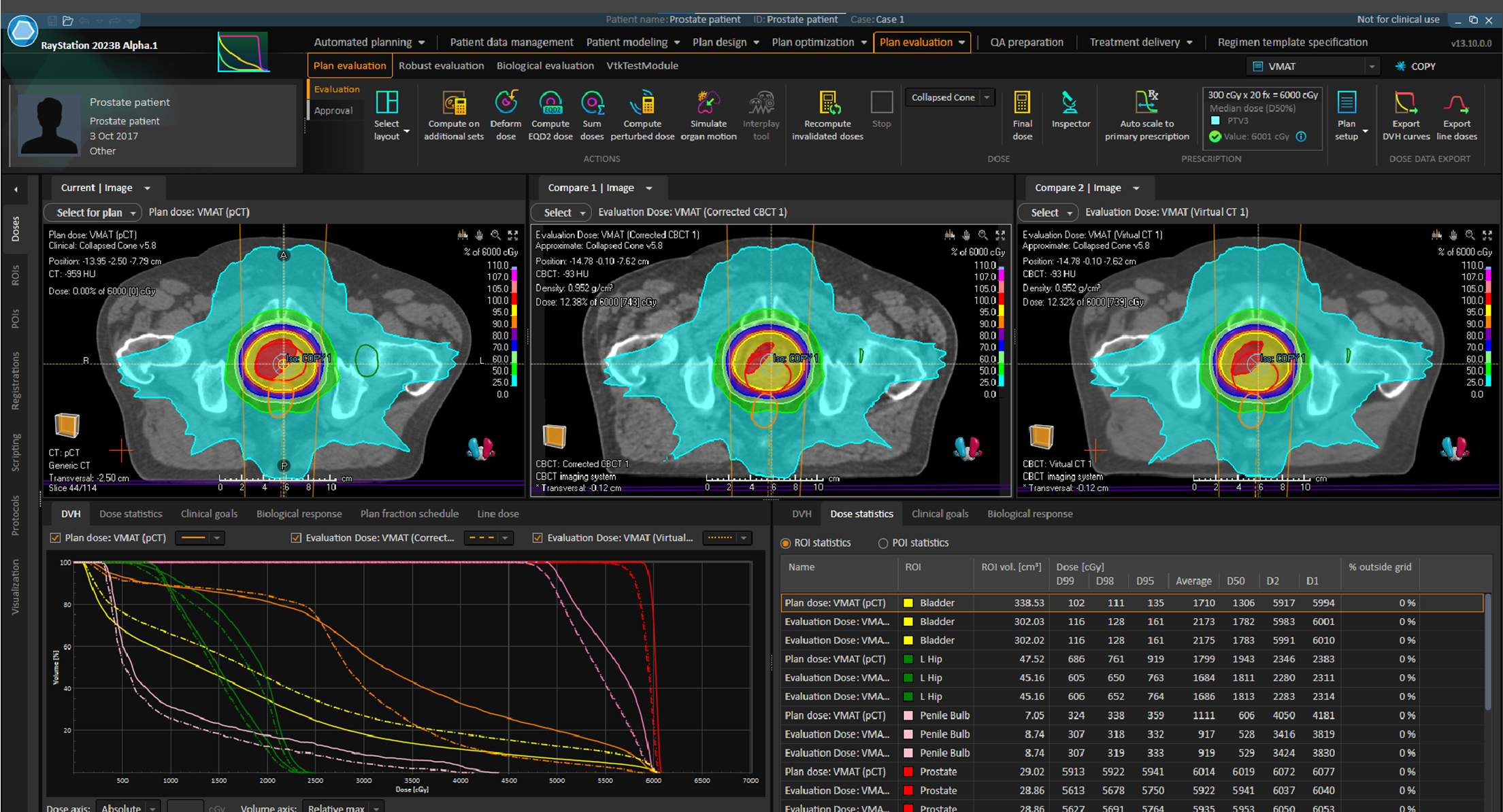
Figure 1. Comparison between the planned dose (left) and the daily fraction dose computed on the Corrected CBCT (middle) and Virtual CT (right). Both synthetic CT algorithms indicate that the plan may need to be adapted, as can be seen in the DVH and dose statistics.
TWO ADVANCED ALGORITHMSTwo algorithms were introduced in RayStation 11B, which create a synthetic CT from the daily CBCT, making it possible to accurately compute dose using HU values instead of using bulk densities. These are included with a rayTracker license, further strengthening the dose tracking and adaptive replanning workflows. |
The Corrected CBCT algorithm works in an iterative manner with two main stages; conversion, and correction. These stages are alternated until convergence. The initial stage finds a conversion from the CBCT intensity scale to the planning CT HU intensity scale, and the second finds a correction map that (for each CBCT voxel) removes low frequency artifacts. This method works for all CBCTs, with no calibration needed and no possibility of changes to the CBCT geometry. In case of limited FOV, parts outside the FOV are copied from the deformed planning CT to the CBCT. |
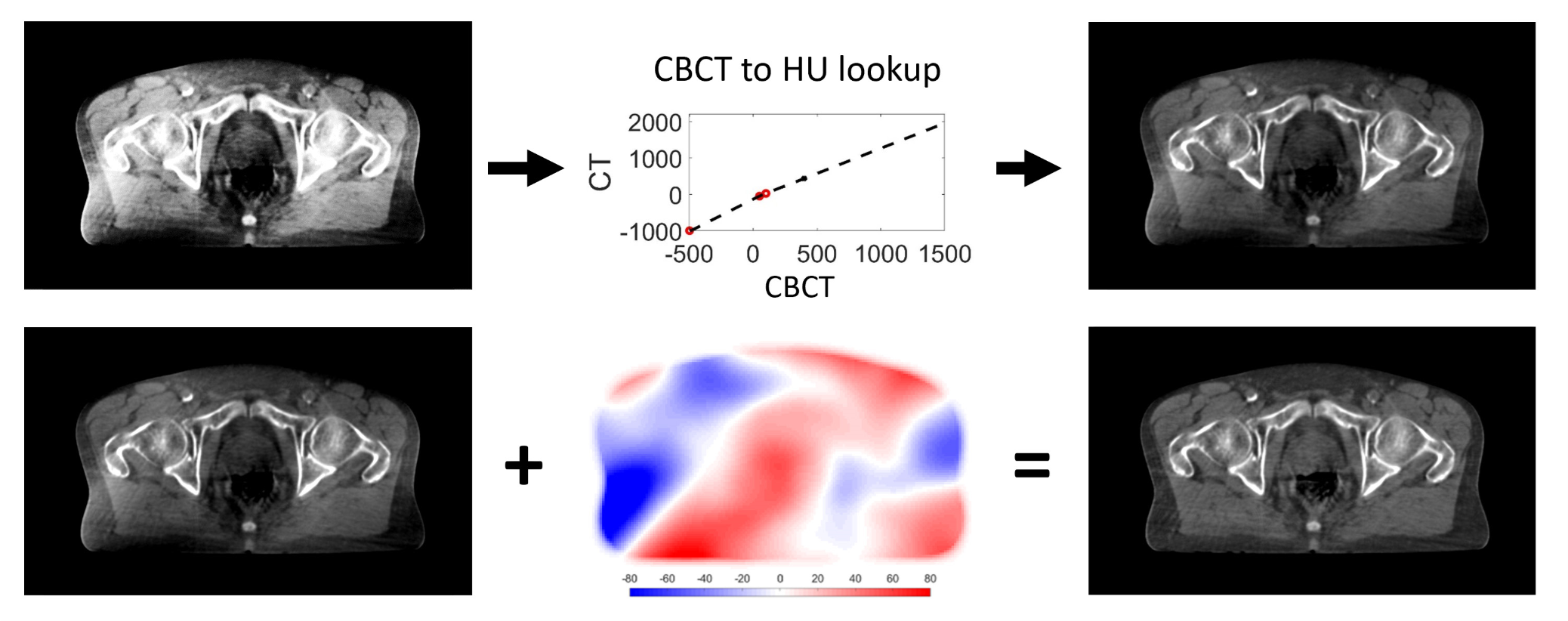
Figure 2. The CBCT is improved iteratively in two stages, none of which alters the patient’s anatomy. In each iteration, a patient specific voxel-vise CBCT value to HU look up table is applied, as well as low frequency (smooth) shading correction map.
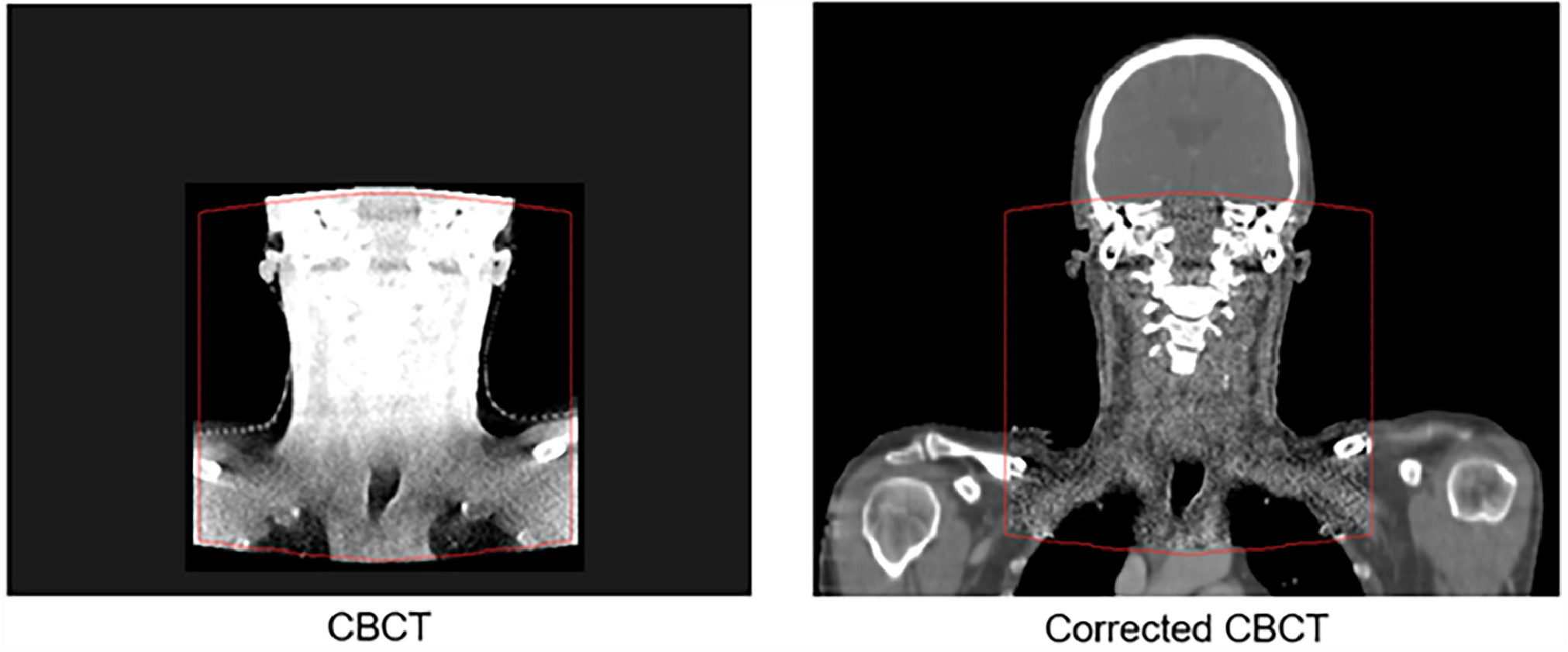
Figure 3. Regions outside of the field-of-view ROI of the CBCT are mapped from the planning CT to the Corrected CBCT using the deformable registration.
The Virtual CT method is a hybrid between a deformed CT and the CBCT correction method. The planning CT is deformed to the CBCT geometry and mismatching low density tissues (air/lung) either in the planning CT or the CBCT, are replaced with values from the corrected CBCT.
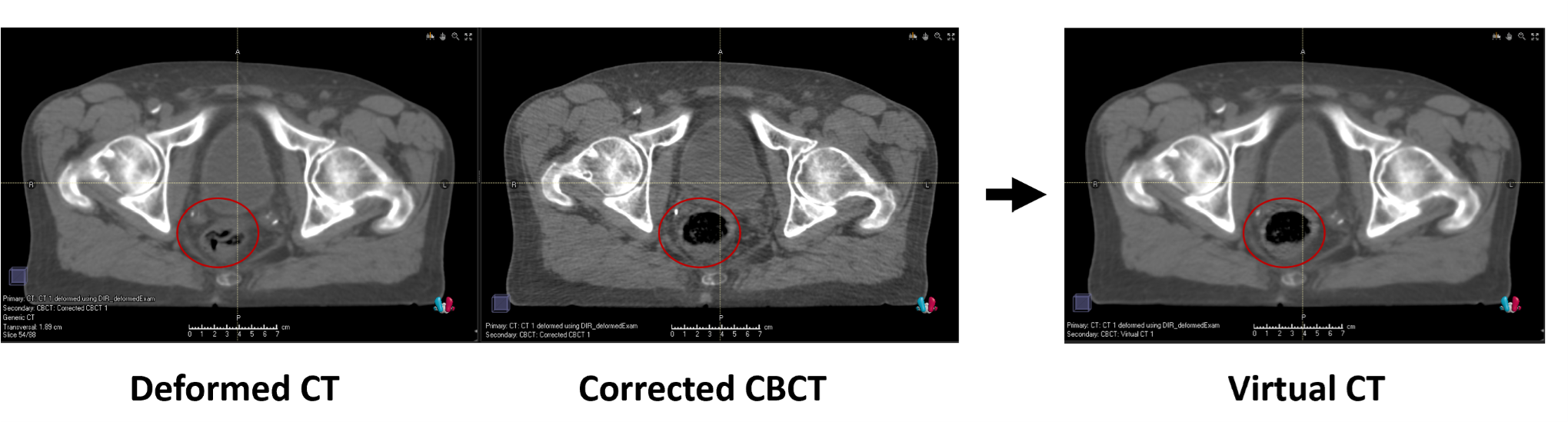
Figure 4. The Virtual CT is created by combining a deformed planning CT and the Corrected CBCT. It takes most of the image from the deformed CT, apart from low density regions such as air or lung that are taken from the corrected CBCT (circled in red).
Why two different algorithms? |
|
|
Corrected CBCT: |
Virtual CT: |
|
If the image quality of the CBCT is sufficient, the corrected CBCT is the preferred option. |
|
|
Rune Slot Thing, Medical Physics Expert, PhD, Vejle Hospital, Denmark |
"Corrected CBCTs have allowed us to evaluate the dosimetric consequences of anatomical changes for all patient groups, faster and more accurately than before. Using scripting, we can create a corrected CBCT, propagate contours and calculate an evaluation dose on the Corrected CBCT within 2 minutes from CBCT import. This workflow allows us to focus our time on the patients where treatment adaptation makes a difference.” |

VALIDATION
The Corrected CBCT and Virtual CT methods have been validated for photons and ions at multiple clinics with good results. 1 In a study by Thing et al.,2 the Corrected CBCT and Virtual CT images show excellent dosimetric agreement with the ground truth CT images. Gamma 2%/2mm pass rates >98% were found for 58/60 thoracic and pelvic patients. DVH similarity to CT within 1% was demonstrated for all pelvic cases, and similarity within +/- 1Gy was shown for all cases. Zhou et al., 3 looked at the feasibility of this method for online evaluation in proton therapy.
Apart from showing good dosimetric agreement, they concluded that online evaluation (from image import to calculated dose) can be achieved within 2 minutes for most clinical proton cases.
SUMMARY/CONCLUSION
CBCT-based synthetic CTs generated by the algorithms in RayStation provide high accuracy in dose computation, a key factor for more reliable and automated workflows for adaptive radiotherapy.
For more information visit:
REFERENCES
[1] References for “The Corrected CBCT and Virtual CT methods have been validated at multiple clinics with good results”
K. Brock et al., “PO-1642: CBCT Padding for Full Field of View Daily Dose Accumulation and Head and Neck Adaptive Radiotherapy,” Radiother. Oncol., vol. 152, pp. S900–S901, Nov. 2020, doi: 10.1016/S0167-8140(21)01660-1.
C. J. O’Hara, D. Bird, B. Al-Qaisieh, and R. Speight, “Assessment of CBCT–based synthetic CT generation accuracy for adaptive radiotherapy planning,” J. Appl. Clin. Med. Phys., Oct. 2022, doi: 10.1002/acm2.13737.
W. Lechner, S. Haupt, D. Kanalas, L. Zimmermann, and D. Georg, “PD-0901 Evaluation of a novel CBCT conversion method,” Radiother. Oncol., vol. 170, pp. S795–S796, May 2022, doi: 10.1016/S0167-8140(22)02980-2.
V. C. Hamming, S. Andersson, J. H. Maduro, J. A. Langendijk, S. Both, and N. M. Sijtsema, “Daily dose evaluation based on synthetic CTs for breast cancer patients: accuracy of dose and complication risk assessment,” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC974617
P. Sabouri, S. Andersson, R. Nilsson, K. Eriksson, and S. Mossahebi, “Using CBCT to Monitor Treatment Dose Delivery Accuracy in Head and Neck Proton Radiotherapy,” Int. J. Radiat. Oncol., vol. 111, no. 3, pp. e150–e151, Nov. 2021, doi: 10.1016/j.ijrobp.2021.07.608.
[2] Evaluation of CBCT based dose calculation in the thorax and pelvis using two generic algorithms R.S. Thing, R. Nilsson, S. Andersson, M. Berg, M.D. Lund Physica Medica 103 (2022) 157–165, https://doi.org/10.1016/j.ejmp.2022.10.012 First published: 31 October 2022
[3] J. Zhou et al., “Cone Beam CT-Based Online Evaluation in Two Minutes Using a Commercial Treatment Planning Software for Proton Therapy,” Int. J. Radiat. Oncol., vol. 111, no. 3, p. e153, Nov. 2021, doi: 10.1016/j.ijrobp.2021.07.614.
*Subject to regulatory clearance in some markets.